


Appendicitis is acute inflammation of the vermiform appendix, typically resulting in abdominal pain, anorexia, and abdominal tenderness. Diagnosis is clinical, often supplemented by CT or ultrasonography. Treatment is surgical removal of the appendix.
(See also Acute Abdominal Pain.)
In the United States, acute appendicitis is the most common cause of acute abdominal pain requiring surgery. Over 5% of the population develops appendicitis at some point. It most commonly occurs in adolescence and in the 20s but may occur at any age.
Other conditions affecting the appendix include carcinoids, cancer, villous adenomas, and diverticula. The appendix may also be affected by Crohn disease or ulcerative colitis with pancolitis (inflammatory bowel disease).
Etiology of Appendicitis
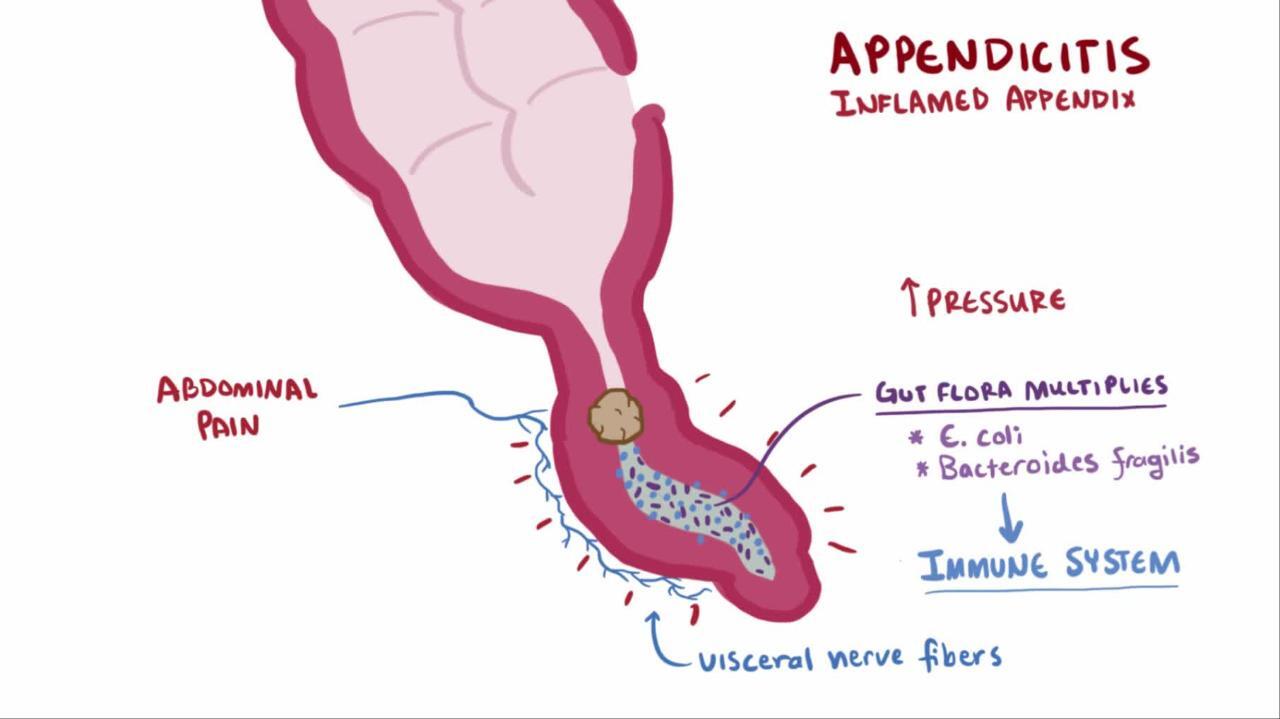
Appendicitis is thought to result from obstruction of the appendiceal lumen, typically by lymphoid hyperplasia but occasionally by a fecalith, foreign body, tumor, or even worms. The obstruction leads to distention, bacterial overgrowth, ischemia, and inflammation. If untreated, necrosis, gangrene, and perforation occur. If the perforation is contained by the omentum, an appendiceal abscess results.
Symptoms and Signs of Appendicitis
The classic acute appendicitis symptoms are
Epigastric or periumbilical pain followed by brief nausea, vomiting, and anorexia
After a few hours, the pain shifts to the right lower quadrant. Pain increases with cough and motion.
Classic signs of appendicitis are
Right lower quadrant direct and rebound tenderness located at the McBurney point (junction of the middle and outer thirds of the line joining the umbilicus to the anterior superior iliac spine)
Additional appendicitis signs are pain felt in the right lower quadrant with palpation of the left lower quadrant (Rovsing sign), an increase in pain caused by passive extension of the right hip joint that stretches the iliopsoas muscle (psoas sign), or pain caused by passive internal rotation of the flexed thigh (obturator sign).
Low-grade fever (rectal temperature 37.7 to 38.3° C [100 to 101° F]) is common.
Many variations of appendicitis symptoms and signs occur in > 50% of patients. Pain may not be localized, particularly in infants and children. Tenderness may be diffuse or, in rare instances, absent. Bowel movements are usually less frequent or absent; if diarrhea is a sign, a retrocecal appendix should be suspected. Red or white blood cells may be present in the urine.
Atypical symptoms are common among older patients and pregnant women; in particular, pain is less severe and local tenderness is less marked.
Diagnosis of Appendicitis
Clinical evaluation
Abdominal CT if necessary
Ultrasonography an option to CT
When classic appendicitis symptoms and signs are present, the appendicitis diagnosis is clinical. In such patients, delaying appendicitis surgery to do imaging tests only increases the likelihood of perforation and subsequent complications.
In patients with atypical or equivocal findings, imaging studies should be done without delay. Contrast-enhanced CT has reasonable accuracy in diagnosing appendicitis and can also reveal other causes of an acute abdomen. Graded compression ultrasonography can usually be done quickly and uses no radiation (of particular concern in children); however, it is occasionally limited by the presence of bowel gas and is less useful for recognizing nonappendiceal causes of pain.
Appendicitis remains primarily a clinical diagnosis. Selective and judicious use of imaging studies may reduce the rate of negative laparotomy.


Laparoscopy can be used for diagnosis as well as definitive treatment of appendicitis; it may be especially helpful in women with lower abdominal pain of unclear etiology. Laboratory studies typically show leukocytosis (12,000 to 15,000/mcL [12.00 to 15.00 × 109/L]), but this finding is highly variable; a normal white blood cell count should not be used to exclude appendicitis.
Treatment of Appendicitis
Surgical removal of the appendix
IV fluids and antibiotics
Treatment of acute appendicitis is open or laparoscopic appendectomy. Because treatment delay increases mortality, a negative appendectomy rate of 15% is considered acceptable.
The surgeon can usually remove the appendix even if perforated. Occasionally, the appendix is difficult to locate. In these cases, it usually lies behind the cecum or the ileum and mesentery of the right colon.
A contraindication to appendectomy is inflammatory bowel disease involving the cecum. However, in cases of terminal ileitis and a normal cecum, the appendix should be removed.
Appendectomy should be preceded by IV antibiotics. Third-generation cephalosporins are preferred. For nonperforated appendicitis, no further antibiotics are required. If the appendix is perforated, antibiotics should be continued for 4 days (1). If surgery is impossible, antibiotics—although not curative—markedly improve the survival rate.
Although several studies of nonoperative management of appendicitis (ie, using antibiotics alone) have shown high rates of resolution during the initial hospitalization, a significant number of patients have a recurrence and require appendectomy during the following year (2). Thus, appendectomy is still recommended, particularly if an appendicolith is visible on CT.
When a large inflammatory mass is found involving the appendix, terminal ileum, and cecum, resection of the entire mass and ileocolostomy are preferable. In late cases in which a pericolic abscess has already formed, the abscess is drained either by an ultrasound-guided percutaneous catheter or by open operation (with appendectomy to follow at a later date).
Treatment references
1. Sawyer RG, Claridge JA, Nathens AB, et al: Trial of short-course antimicrobial therapy for intraabdominal infection. N Engl J Med 372(21):1996–2005, 2015. doi: 10.1056/NEJMoa1411162
2. Poon SHT, Lee JWY, Ng KM, et al: The current management of acute uncomplicated appendicitis: Should there be a change in paradigm? A systematic review of the literatures and analysis of treatment performance. World J Emerg Surg 12:46, 2017. doi: 10.1186/s13017-017-0157-y
Prognosis for Appendicitis
Without surgery or antibiotics, the mortality rate for appendicitis is > 50%.
With early surgery, the mortality rate is < 1%, and convalescence is normally rapid and complete.
With complications (rupture and development of an abscess or peritonitis) and/or advanced age, the prognosis is worse.
Key Points
Patients with classic symptoms and signs should have laparotomy instead of imaging tests.
Patients with nondiagnostic findings should have imaging with CT or, particularly for children, ultrasonography.
Give a 3rd-generation cephalosporin preoperatively and, if the appendix has perforated, continue it postoperatively.






